
|
Every is likely aware of the conventional advice to treat shin splints: R.I.C.E., stretching, a switch to softer running surfaces, training plan modifications, maybe a new pair of shoes or a change in running technique. While each of these techniques have merit as treatment approaches, sometimes you need to think a little outside stay on your feet with minimal disruption in training. Now, before we treat "shin splints" it is important to confirm that shin splits are really what we're dealing with. For purposes of this article, we'll associate the term shin splints the diagnosis of medial tibial stress syndrome ("MTSS"). In the popular lexicon, shin splints are frequently associated with a myriad of diagnoses including anterior compartment syndrome, anterior tibial tendonitis and stress fractures or stress reactions, among others. The shin splints we'll discuss here involve pain along the inside of the shin as shown below. 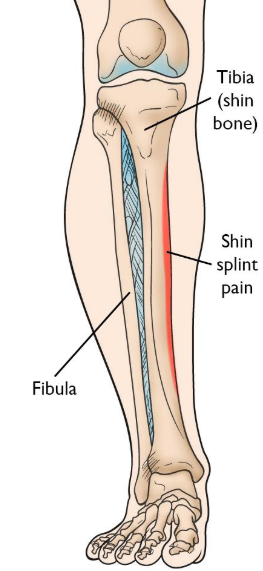 One technique that you've probably seen elsewhere on the body but perhaps not on the shin is kinesiotaping. A recent study by Griebert (2016) measured rate of loading both with and without kinesiotaping on the medial shin area of subjects with a present or past history of shin splints, and found that kinesiotape reduced the the stress placed on the area after 24 hours of continuous use. Another study by Kachanathu (2018) compared kinesiotaping with orthotics for shin splint treatment and found that kinesiotaping was more effective at reducing pain and improving functional performance, as measured by a single leg hop test. There are several specific taping techniques available but here is one very simple one from Rocktape... Another technique is Instrument Assisted Soft Tissue Mobilization (IASTM), which can be helpful to access some harder to reach areas of the front and inside of the shin, but more importantly, can help create better mobility throughout the lower leg to help "off-load" stress upon the shin splint area. This is one key point that should guide any thought process: our goal is not simply to treat the painful area (though that can be important for symptom control and short term quality of life), but instead, give the brain and body additional movement alternatives to whatever stride pattern is causing the problem. The "faulty" stride might be the body's only way to move in the presence of other limitations. I won't go too much into IASTM for the posterior leg, or calf muscles, since those techniques are more well known. But I will share one technique example that can provide symptom relief on the front of the shin, particularly when fingers have a more difficult time accessing a particular area. Similar to IASTM, cupping can provide access to harder to reach areas of tissue on the inside of the shin. I like Rockpods for this area given their small size, which makes them appropriate for this area.. CONCLUSION
It is important to recognize that none of the treatments shown here are intended to be "standalone" interventions. That is, they should be performed in combination with interventions to improve mobility, stability and coordination. Unfortunately, if we don't achieve some immediate symptom improvement, we might never get to the more potent exercise interventions. Think of these interventions as methods to create a window of opportunity that allow you to perform the ACTIVE (not passive) approaches most critical for lasting rehabilitation. Allan Phillips, PT, DPT Oro Valley, Arizona physical therapy
1 Comment
1/25/2022 07:44:24 pm
The biggest low-temperature thermoplastic splints and radiotherapy masks manufacturer in Canada. We provide various sizes, colors, perforated thermoplastic splints Radiotherapy Mask, Allfit Nasal Casts, Thermoplastic Brace at attractive prices. Leave a Reply. |
AuthorAllan Phillips, PT, DPT is owner of Ventana Physiotherapy Archives
December 2023
Categories
All
|
 RSS Feed
RSS Feed
2951 N. Swan Rd.
Suite 101, inside Bodywork at Onyx
Tucson, Arizona 85712
Call or Text: (520) 306-8093
[email protected]
Terms of Service (here)
Privacy Policy (here)
Medical disclaimer: All information on this website is intended for instruction and informational purposes only. The authors are not responsible for any harm or injury that may result. Significant injury risk is possible if you do not follow due diligence and seek suitable professional advice about your injury. No guarantees of specific results are expressly made or implied on this website.
Privacy Policy (here)
Medical disclaimer: All information on this website is intended for instruction and informational purposes only. The authors are not responsible for any harm or injury that may result. Significant injury risk is possible if you do not follow due diligence and seek suitable professional advice about your injury. No guarantees of specific results are expressly made or implied on this website.
Proudly powered by Weebly