
|
“Shin splints” is one of those broad terms that many people (doctors included) use to describe a very wide range of conditions. In other words, if someone says “shin splints” what they actually mean can be several different things.
Going “by the book,” shins splints is synonymous with “medial tibial stress syndrome” which is basically irritation at the connection between muscle (usually the posterior tibialis) and the tibia (shin bone). Tends to be a repetitive strain condition, but can have underlying causes in mechanics, strength, mobility or training load; or in the case of bone injuries there can be nutrition causes as well. Occasionally, the irritation might be on the muscle itself without any irritation to the bone, in which case it would be some form of posterior tibialis strain or tendinopathy of the posterior tibialis tendon, if closer to the ankle. As for bone injuries, we can have a stress reaction or a stress fracture. The difference is these is basically one of degree. Think of a stress reaction as the beginnings of a stress fracture. Whereas a stress reaction might dissipate within days if given time to heal, a full blown stress fracture can know you out of a solid couple of months. The hallmark sign will be pain/tenderness in a specific spot, whereas many other shin conditions will display pain along a longer segment. On the outside of the shin on the more “meaty” muscle side, we can have anterior tibial tendinopathy or tibialis anterior strain. You may also hear the term “compartment syndrome” which gets tossed around quite liberally referring to pain on the outside of the shin, but full blown compartment syndrome is a true medical emergency, where you’ll experience numbness, loss of circulation and changes to skin texture. The gold standard to diagnose compartment syndrome is to measure the pressure inside the compartment. Sometimes, shin pain isn’t shin pain at all, but is instead nerve pain from the lower back. You could also experience nerve-like symptoms from irritation at the outside of the knee. But in these scenarios, the symptoms are less likely to be associated with movements or direct stress to the lower leg. High ankle sprain is also slim possibility, but unless you’ve had an acute incident of twisting your ankle or lower leg, it’s safe to rule this one out. Ultimately, these diagnoses are simply descriptive labels. Most important is identifying how and why these are happening, but understanding that many different conditions can exist under the realm of “shin splints” is a good way to start! “What’s harder..Road marathon or trail ultramarathon?” I’ll start by saying neither is “harder” than the other; both are more challenging in their own right. I will say that marathon is a more intense pain but that’s only one metric of “harder.” The marathon inflicts the punishment of repetitive strain being on the road for 26.2 miles, basically using the same muscles in the same way for hours. Some mild hills can create some variety, but that can also make the course slower (we’re assuming that the goal is to compete the courses in your fastest possible time). If the hills get too big, they can punish your quads on the downhills. But regardless, you can expect your legs to be VERY sore after a full effort road marathon, especially if part of the course takes you to concrete. The intensity of the road race is also higher as most competitive runners are working toward the upper half of their aerobic energy system. In the ultra, I was sore but not nearly as sore as after road marathons. To an extent, this shouldn’t be surprising because the ultra included bouts of walking during some uphills when I caught up to people on a single track and also when going through the later aid stations. Additionally, most ultras are contested mainly on soft surfaces, which inflicts less pounding. Add in the technical nature of many ultra courses and you have a recipe to spare your legs a bit…even though you have more ground to cover than on the road.  Some notes for a Zoom Q&A session where I was a guest of Run Tucson and The Workout Group 1. Why is adding some strength into your routine helpful for running? Strength makes more adaptable as human beings. We are constantly exposed to stressors, some good, some not so good, and improving the physical as well as mental quality of strength provides a better internal ecosystem within our body to make appropriate adaptations to those stressors…the stress of pounding the pavement the skill of making corrections on the trail, reversing the pulls of office life, the natural biological processes that occur with aging (loss of muscle, loss of tissue elasticity) counteracting the catabolic (tissue wasting) processes that accompany moderate to high volume aerobic training Historical evidence: the clusters of populations that have been successful over time have all had some basis in strength training practice. "Old school" Americans came from active lifestyle and many worked manual jobs at some point in their lives; many of the the African runners work in agriculture and have minimal access to motorized vehicles; Japanese runners enjoy very robust physical education programs in their youth 2. Are activation and stability exercises considered strength training? Yes, but for most people in the same way that mashed potatoes and asparagus fit into a meal with a steak. They’re food but they are side dishes. You can still get an adequate meal by ordering off the appetizer and sides menus and that might be all you need at the time.(Or its like a Clif Bar or gel pack aren't the same as a complete meal but in the right time and place they’re more appropriate for the situation than a giant steak.) So yes activation fits under that broad umbrella category of strength but it’s important to appreciate their proper context and limit yourself at activation exercises when you can still benefit from taking it a step further into strength training. Ultimately, activation and stabilization are prerequisites for quality movement. When we’re assessing the strength of an individual muscle, the scale runs from simply asking whether the muscle can actually activate all the way up to can it move our body against gravity and external resistance. Its all the same scale, just all part of a continuum. For a lot of things where we are highly proficient, something in the realm of activation or stability might not be an adequate load or stimulus to improve strength. But for some areas where we might be less developed or proficient, such as lateral movements, simply activating or stabilizing against a modest load might be all the stimulus you need to be challenged. But in the end its all part of the same neurological processes 3. How should someone start adding strength into their routine? Conduct a needs analysis – are you historically injured and maybe have done some strength associated with rehab but just never stuck with it? Are you historically healthy and just want make sure your bases are covered? The answers to these types of questions will help guide you to YOUR best starting point. Set up your environment for success – we’re in a unique situation right now where involving the family in a fitness routine is a very positive development, both for enjoyment and accountability Start with your running schedule and work backward from there Easy victories – Don’t have to be on some elaborate plan, especially if you’re starting from basically scratch  4. If you could pinpoint 5 strength exercises that are the most helpful for runners, what would they be?
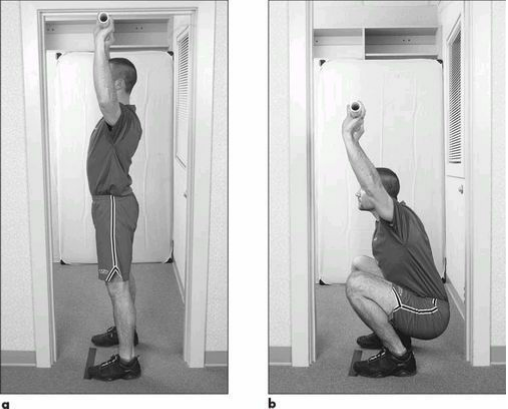
Strive to include an exercise from each of these categories. The specific exercises will be different for everyone, but these are the key movements to focus on. The examples provided are some of my preferences, but there are many options to choose from. Pull - pull ups, rows Push - overhead pressing, push ups Hinge - single leg deadlift, glute bridge Squat - split squat, goblet squat Core - plank, Turkish getup 5. Can runners over-do it when it comes to strength training? Absolutely! But the effects are typically subtle and the effect can be be delayed for several days or weeks Biggest problem I see isn't overdoing it in an absolute sense, but in a relative sense. Most of the time when runners overdo it, the overdone program wouldn't be too much if they weren't also serious about running. Usually, the error is failing to protect quality run days from interference of lower body strength work. The magic, the essence of any training approach isn’t what we decide to do or what the coach decides to do…its what we choose to NOT do… 6. Is there anything we should stay away from? Compressing or cutting out the rest periods. Shortening the rest sounds like a good idea and feels natural for an endurance athlete.... "lets save time and be efficient" or "it really feels like I’m getting after it because my heart rate is up" or "I can't stand waiting around between exercises for a couple minutes." This thinking also drives many commercial models based on HIIT training or some form of circuit training. There can be value in these when presented a certain way, but the more we shorten the rests, the more we deviate from actual strength training. If you need more endurance, then look to your running program, don’t try to create something in the gym. This is hardly an exhaustive list, but these are just a few of my favorites. Please share your favorites in the comments if not covered in here. And feel free to share your own perspective on any that I did cover! Reid Park – Definitely the most popular run spot in town. The main loop is the nearly three mile loop around the golf courses, which is marked every quarter mile and has the full three mile mark shortly past the “Start.” Definitely a good spot for all types of workouts, both measured as well as fartleks. Overall fairly flat, with a slight incline from mile 0.5 to 1.0 and 2.0 to 2.5-ish. Generally is well guarded from the wind compared to other flattish trails in town. No bathrooms right at the start of the main loop but plenty of bathrooms scattered throughout the park. Along with the main loop, there is an additional paved loop that continues around the baseball/zoo/park areas. You can also make a grass/dirt run through the middle of the park. During cross country season, there’s actually a marked course that you can follow. Finally, although the track is locked to the public outside of organized training groups, the 800m loop around the baseball field warning tracks is one of the best “tracks” you’ll find for workouts! Throughout the year you can find several races that utilize part of the path and the surrounding area. 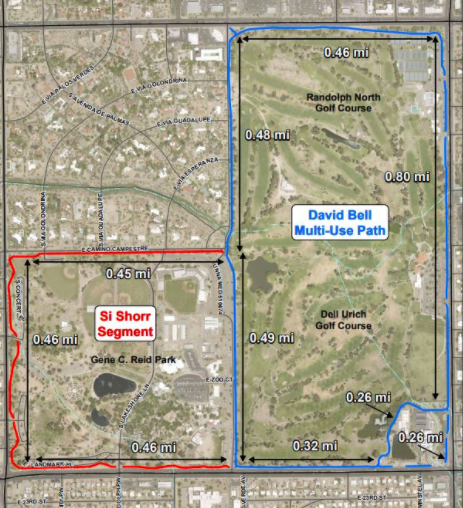 Here's a very simple movement assessment that I often recommend to people that you can complete on your own. This five part assessment has been around since the 1990s and is something I've used remotely with athletes for years. But with the shift of more training and treatment into the virtual space, this assessment and others like it are becoming more integral pieces of the training process. Originally appearing in Gray Cook's Athletic Body in Balance, this assessment looks at five movement patterns: an overhead deep squat, hurdle step, inline lunge, active straight leg raise and trunk rotation. You may recognize a form of these from the Functional Movement Screen. Other than some small details in execution, the main difference is these are graded on a PASS/FAIL basis. The purpose here is not to dissect movement into minute details but instead to have a way to quickly determine if someone has major gaps that we need to identify before exploring heavier loads (which can take the form of additional weight, speed or complexity). There are plenty of different ways to assess remotely, but I have found this one to seamlessly transition into the next phase of the training process. You might wonder," only five PASS/FAIL moves, how can that be of any value?" Remember this is simply a starting point that guides us to the next step, whether that is getting after it in training or doing more detailed assessments of particular results (that might otherwise be unneeded in some individuals). Throwback Thursday!....This month marks the ten year anniversary of my marathon PR run at the Eugene Marathon in Eugene, Oregon (aka Tracktown USA). The place oooozes with running history and even if this had not been a PR performance the trip still would have been a massive success. What follows is a recap of the race itself and my training leading up to it...  Bottom line: If you have an injured limb and are unable to train as normal (or train at all), training the other side can still yield benefits of the injured side Question time….Let’s say you injure your left knee. What is the best strategy for your training plan? 1 Push through pain no matter how bad it is. Don’t change your training plan. Rest is for sissies 2 Continue to train the right knee, so long as it doesn’t further injure or provoke symptoms in the left 3 Stop training both legs because you don’t want you’re right leg to become too strong relative to your left and develop an asymmetry There is a “best” answer here and that answer is number 2. Answer number 1 is ridiculous, so we’ll put that one aside. Number 3 sounds compelling and while it wouldn’t necessarily be “wrong” to go that direction, there are several reasons why number 2 is better. Again, this is all based on the caveat that the training you do for the uninjured limb doesn’t put the injured limb at further risk of injury or delay healing. For example, let’s say you were doing some single leg activities on the uninjured leg, but each impact sent a “shock” through the injured leg. Your best bet is to either find different activities or delay training the uninjured limb until it can be done safely without provoking the injured limb. In the literature, the concept of training effects on one limb being felt on the opposite side limb is called cross education. And to the surprise of some, the evidence is quite clear that cross-education works. Unfortunately, what should be the standard of care (training the rest of the body at the highest level possible in a way that supports the healing process), is instead a novel concept to many.  There are several reasons why cross-limb education is not promoted more. One is that the medical process is often siloed and sees the world with tunnel vision. For example, most orthopedic surgeons are going to just look at the injury and not even consider. That’s not meant to be critical, it’s just the nature of their job. They’re good at going into a damaged body part and making structural corrections using surgical techniques. They aren’t paid to tell you how to train. Similarly, most PT’s in a “traditional” outpatient setting aren’t getting paid to consider the opposite leg (and in some cases are actively discouraged from looking anyplace other than the site of the injury…Not their fault, that’s just the nature of the system in which they work). uninjured limb.
What does the evidence say?....A meta-analysis by Green (2018) reviewed 96 studies on cross education involving healthy young adults, healthy older adults and patients, finding an average strength gain via cross education of 18% in young adults, 15% in older adults, and 29% in a patient population. Although prior meta analyses had shown conflicting results on gender differences and upper versus lower limb effects, the studies compiled by in the Green meta-analysis revealed no significant differences. Overall, the average cross body transfer ranged from 48%-77% in the compiled studies, meaning that the immobilized limb experienced strength gains of 48%-77% of the trained limb. Again, this isn’t just one study on a homogenous group of subjects…this is 96 studies in a variety of populations. (Another interesting finding was that electrically stimulation of muscles appeared to have a greater cross-education effect than voluntary stimulation). WHY cross education works remains up for debate but most evidence points to neurological mechanisms as the primary factors. Per Cirer-Sastre (2017), “this owes to the fact that no significant vascular adaptations have been found, nor were any histological changes in hypertrophy levels, in enzyme concentration, in contractile protein composition alteration, in fiber type or in cross-sectional area.” In short, strength is function of the nervous system, and the effects of nervous system output are global, meaning not specific to any single body part. Although the evidence has been relatively settled that cross-education does exist via single sided training, HOW to facilitate cross-education is less clear although a meta-analysis of ten studies by Cirer-Sastre, “to optimize contralateral strength improvements, cross-training sessions should involve fast eccentric sets with moderate volumes and rest intervals. Finally, approaching this from a pragmatic standpoint, if you sustain an injury to a limb, you could continue training the other limbs and have three “good” limbs or you could stop training both the injured and non-injured arm/leg and have two “good” limbs. Which sounds better? The concern about developing asymmetries is logical, but overall is far overblown. As we know from the research, the cross-education effect will mitigate strength losses from inactivity by an injured limb. Further, even if cross-education did not exist, you’re better off having to bring one limb up to speed rather than losing strength in both sides have having two limbs to return to normal. Simply makes no sense why you would voluntarily weaken a perfectly healthy limb. Even if an asymmetry develops during a recovery period, its not as though you were going to hop right back into peak training after you get over the injury. You might as well give yourself the highest “baseline” with a strong, healthy limb rather than let both sides regress. REFERENCES Lara A. Green & David A. Gabriel (2018) The effect of unilateral training on contralateral limb strength in young, older, and patient populations: a meta-analysis of cross education, Physical Therapy Reviews, 23:4-5, 238-249, DOI: 10.1080/10833196.2018.1499272 Cirer-Sastre R, Beltrán-Garrido JV, Corbi F. Contralateral Effects After Unilateral Strength Training: A Meta-Analysis Comparing Training Loads. J Sports Sci Med. 2017;16(2):180–186. Published 2017 Jun 1. History of Graston Technique… David Graston was competitive water skier; sustained injury but frustrated with poor results from other treatments; went and used jar top as a self massage tool and improved; used his engineering knowledge to create specialized instruments, hence the birth of Graston Technique More than just scraping and making the skin red (people often associate Graston with these giant bruises, but contemporary thinking has evolved quite significantly).. Many variables to consider for best possible treatment…size of instrument, which treatment edge, shape of body part being treated, speed of stroke, length of stroke, type of stroke, target tissue length, angle of instrument edge, treatment duration… I did go in without an intention of purchasing the instruments….but I ended up getting them anyway (in full disclosure, the military and student discounts did play a role in my decision to ultimately purchase)  |
AuthorAllan Phillips, PT, DPT is owner of Ventana Physiotherapy Archives
December 2023
Categories
All
|



 RSS Feed
RSS Feed
2951 N. Swan Rd.
Suite 101, inside Bodywork at Onyx
Tucson, Arizona 85712
Call or Text: (520) 306-8093
[email protected]
Terms of Service (here)
Privacy Policy (here)
Medical disclaimer: All information on this website is intended for instruction and informational purposes only. The authors are not responsible for any harm or injury that may result. Significant injury risk is possible if you do not follow due diligence and seek suitable professional advice about your injury. No guarantees of specific results are expressly made or implied on this website.
Privacy Policy (here)
Medical disclaimer: All information on this website is intended for instruction and informational purposes only. The authors are not responsible for any harm or injury that may result. Significant injury risk is possible if you do not follow due diligence and seek suitable professional advice about your injury. No guarantees of specific results are expressly made or implied on this website.
Proudly powered by Weebly